Imagine waking up one morning to find that half of your face has gone completely numb. You try to smile, but only one side moves. You can’t close one eye, and water spills from your mouth when you drink. It is a terrifying experience, but it might not be a stroke. This sudden onset of unilateral facial weakness is the hallmark of Bell’s palsy, which is an idiopathic facial nerve paralysis characterized by acute onset and no identifiable cause after thorough examination. While the condition sounds alarming, the good news is that most people recover fully. The key difference between a full recovery and lasting damage often comes down to one specific intervention: starting corticosteroid therapy within the first 48 hours.
First described by Scottish surgeon Sir Charles Bell in 1821, this neurological disorder affects approximately 15 to 30 people per 100,000 annually. The peak incidence occurs between ages 15 and 45, meaning it can strike anyone in their prime. Without treatment, about 70% of patients still recover spontaneously. However, with the right medication, those odds improve significantly, and the risk of permanent complications drops sharply. Understanding why steroids work and how to use them correctly is the most important step you can take if you suspect you have this condition.
The Mechanism: Why Steroids Save the Nerve
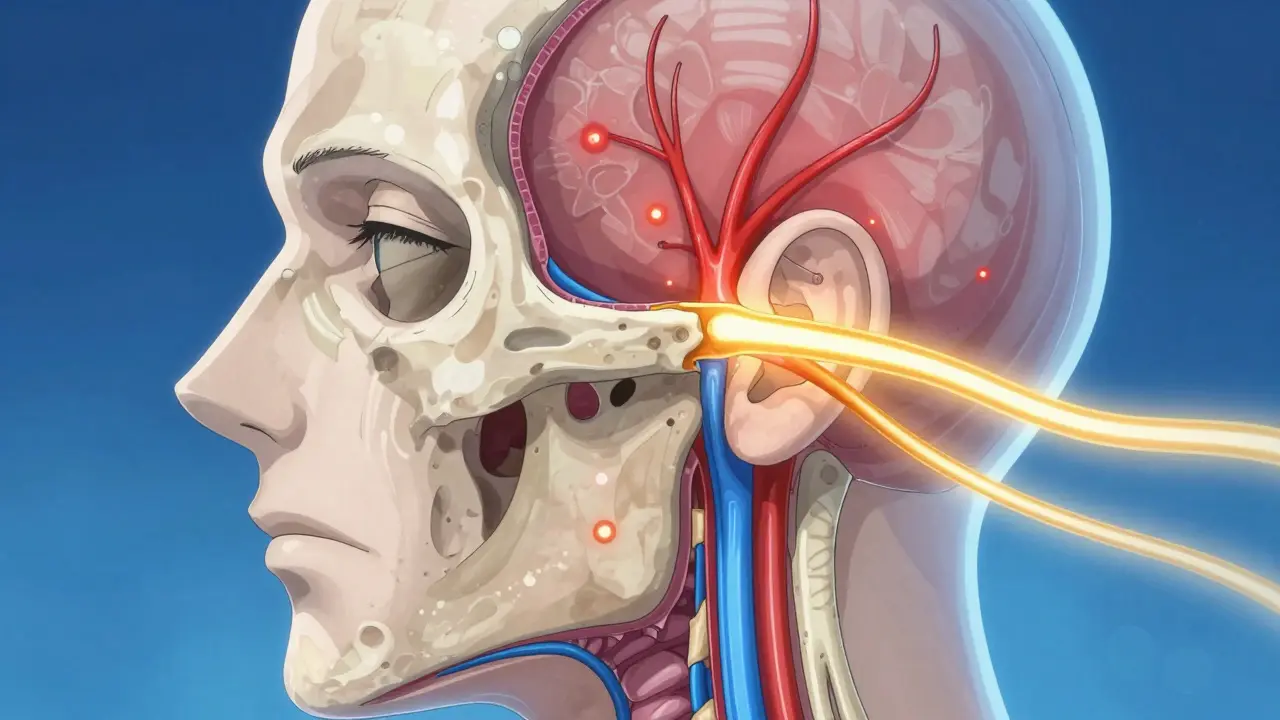
To understand why corticosteroids are the gold standard, we need to look at what happens inside your head. The facial nerve, also known as cranial nerve VII, travels through a narrow bony tunnel called the fallopian canal. When Bell’s palsy strikes, inflammation causes the nerve to swell. Because the canal is so tight, the swelling compresses the nerve against the bone, cutting off blood supply and disrupting signals to your facial muscles.
Corticosteroids, such as prednisone, are powerful anti-inflammatory agents. They work by reducing this edema (swelling) quickly. By shrinking the inflammation, they relieve the pressure on the nerve before permanent damage occurs. Think of it like a kinked garden hose; the steroid removes the kink, allowing flow to resume. The Cochrane Database of Systematic Reviews (2019) provides high-quality evidence showing that this mechanism significantly reduces the rate of incomplete recovery. Specifically, the relative risk of poor outcomes drops by nearly 31% when steroids are used compared to placebo.
The Critical Window: Timing Is Everything
If you notice facial drooping, do not wait. The effectiveness of corticosteroids is heavily dependent on timing. Clinical data indicates that initiating treatment within 48 hours of symptom onset yields the best results. Some benefit remains if you start within 72 hours, but after that window closes, the drug’s ability to prevent nerve damage diminishes rapidly.
Why is this window so short? Because nerve compression can lead to irreversible ischemia (lack of blood flow) relatively quickly. Once the nerve fibers die, no amount of anti-inflammatory medication can bring them back. This is why delayed diagnosis is a major issue. Many patients wait three days or more to see a doctor, hoping the symptoms will resolve on their own. This delay costs them precious time. If you live in Adelaide or anywhere else, seek immediate medical attention. Do not assume it will pass. Early intervention is the single most controllable factor in your recovery journey.
Dosing Protocol: More Is Not Always Better, But Enough Is Essential
When doctors prescribe steroids for Bell’s palsy, they follow a specific protocol designed to maximize efficacy while minimizing side effects. The standard regimen, supported by the American Academy of Family Physicians (AAFP), involves oral prednisone at a dose of 50 to 60 mg daily for five days, followed by a five-day taper. This results in a total cumulative dose of approximately 500 mg over ten days.
Research shows a clear dose-response relationship. A cumulative dose of less than 450 mg is associated with a 30% rate of unsatisfactory recovery, whereas doses of 450 mg or higher drop that rate to just 14%. This means taking the full prescribed course is crucial. Stopping early because you feel better or worry about side effects can undermine the treatment. The number needed to treat (NNT) is 10, meaning for every 10 patients treated with this protocol, one case of incomplete recovery is prevented. That is a statistically significant clinical benefit.
| Treatment Strategy | Recovery Rate (Approx.) | Evidence Quality | Key Benefit/Risk |
|---|---|---|---|
| No Treatment | 70% | High | Risk of permanent synkinesis |
| Corticosteroids Alone | 80-90% | High | Reduces incomplete recovery by 31% |
| Antivirals Alone | No significant improvement | Moderate | Not recommended as monotherapy |
| Steroids + Antivirals | Similar to steroids alone | Moderate | May reduce synkinesis rates slightly |
Steroids vs. Antivirals: Clearing Up the Confusion
You might hear conflicting advice about antiviral medications. Some doctors add acyclovir or valacyclovir to the steroid prescription, believing that viruses like herpes simplex trigger the inflammation. However, the evidence does not strongly support using antivirals alone. In fact, antiviral monotherapy shows no significant benefit over placebo.
Combination therapy (steroids plus antivirals) is a nuanced topic. Moderate-quality evidence suggests it may help reduce the rate of synkinesis-a condition where facial muscles move involuntarily together during recovery-but it does not necessarily improve overall recovery rates compared to steroids alone. The AAFP assigns a rating B to combination therapy, suggesting it should be considered, particularly for severe cases. However, for the average patient, steroids remain the primary driver of success. Do not skip the steroids to take antivirals; the opposite would be a mistake.
Side Effects: Managing the Short-Term Trade-Off
A common fear among patients is the idea of "steroid side effects." People associate long-term steroid use with weight gain, osteoporosis, and immune suppression. However, the 10-day course for Bell’s palsy is short enough that these chronic risks are negligible. The real-world side effects are usually mild and temporary.
Patient reports and clinical trials highlight issues like increased appetite, mood changes, difficulty sleeping, and temporary sleep disturbances. For diabetic patients, blood glucose levels may spike during the 10-day course, requiring closer monitoring. Despite these minor inconveniences, studies involving hundreds of participants found no significant difference in serious adverse events between steroid users and placebo groups. The benefits of saving your facial function far outweigh the discomfort of a few bad nights’ sleep or a slight change in mood.

Prognosis and Recovery Metrics
How do doctors measure if you are getting better? They use standardized tools like the House-Brackmann Facial Nerve Grading System. This scale ranges from Grade I (normal function) to Grade VI (total paralysis). Recovery is defined as returning to Grade I or II.
With appropriate treatment, machine learning analyses of large patient datasets show that 72.6% of patients recover fully within three months, and 89.5% recover within nine months. Age is the other biggest predictor of recovery; younger patients tend to heal faster. If you are under 45 and start steroids within 48 hours, your prognosis is excellent. Even if you don’t recover immediately, patience is key. Nerves heal slowly.
Practical Steps for Patients
If you suspect Bell’s palsy, here is your action plan:
- Seek Immediate Care: Go to a clinic or emergency room within 24-48 hours of symptom onset. Rule out stroke first.
- Start Steroids Promptly: Ensure you receive a prescription for prednisone or an equivalent corticosteroid. Confirm the dosage is around 50-60 mg initially.
- Protect Your Eye: Since you may not be able to blink, use artificial tears during the day and ointment at night. Tape the eye shut while sleeping to prevent corneal damage.
- Adhere to the Taper: Take the full 10-day course, even if your face starts looking normal after three days.
- Monitor Blood Sugar: If you are diabetic, check your glucose levels more frequently during treatment.
Telemedicine platforms have made it easier to get assessed quickly. In some regions, video consultations can expedite prescriptions, reducing the delay caused by waiting for in-person appointments. Utilize these resources if physical access to a doctor is slow.
Can Bell's palsy be cured permanently?
Yes, the majority of patients experience full recovery. With corticosteroid treatment, approximately 80-90% of people regain complete facial function. Most recovery happens within three to nine months.
Is Bell's palsy contagious?
No, Bell's palsy itself is not contagious. While viral infections may trigger the inflammation, the paralysis is a local reaction in the nerve, not an active infection you can spread to others.
What is synkinesis?
Synkinesis is a complication where facial muscles reconnect incorrectly during healing. For example, your eye might close when you try to smile. Early steroid treatment helps reduce the risk of this occurring.
How long does the steroid treatment last?
The standard course is 10 days. This typically involves 5 days of high-dose prednisone (50-60 mg) followed by a 5-day tapering schedule to lower the dose gradually.
Can stress cause Bell's palsy?
Stress does not directly cause Bell's palsy, but it may weaken the immune system, potentially making you more susceptible to the viral reactivation that triggers the condition. However, the exact cause remains idiopathic (unknown) in many cases.