Imagine your liver slowly turning into a hard, scarred sponge that can no longer filter toxins from your blood. That is exactly what happens in cirrhosis, which is the final stage of chronic liver disease where healthy tissue is replaced by non-functional scar tissue. It is not just a minor health hiccup; it is a serious condition that affects how your entire body functions. Many people live with early-stage cirrhosis without knowing it because the liver is remarkably good at hiding damage until it is too late. By the time symptoms like swelling or confusion appear, the disease has often progressed to a critical point.
Understanding this condition is vital because the difference between living a normal life and facing a life-threatening crisis often comes down to early detection and proper management. This article breaks down what cirrhosis really is, why it happens, how doctors measure its severity, and what options exist when the liver fails completely, including transplantation.
What Is Cirrhosis and How Does It Develop?
To understand cirrhosis, you first need to understand how the liver heals itself. When your liver cells are damaged-whether by alcohol, viruses, or fat buildup-the liver tries to repair the injury. It does this by producing collagen, a fibrous protein that forms scar tissue. In small amounts, this scarring is part of the healing process. But if the damage continues over years, the scar tissue spreads. Eventually, these scars block blood flow through the liver and replace healthy cells that perform essential tasks like detoxifying blood and producing proteins.
This process is called fibrosis. When fibrosis becomes widespread and permanent, distorting the liver’s structure, it is diagnosed as cirrhosis. The term comes from the Greek word 'kirrhos,' meaning tawny yellow, referring to the discolored appearance of a diseased liver. Unlike earlier stages of liver disease, such as fatty liver or hepatitis, cirrhosis is generally considered irreversible. Once the architecture of the liver is destroyed, it cannot regenerate back to its original healthy state. However, stopping the cause of the damage can prevent further scarring and keep the remaining liver functioning for many years.
The Two Stages: Compensated vs. Decompensated
Doctors classify cirrhosis into two main stages based on how well the liver is still working. Knowing which stage you are in determines your treatment plan and outlook.
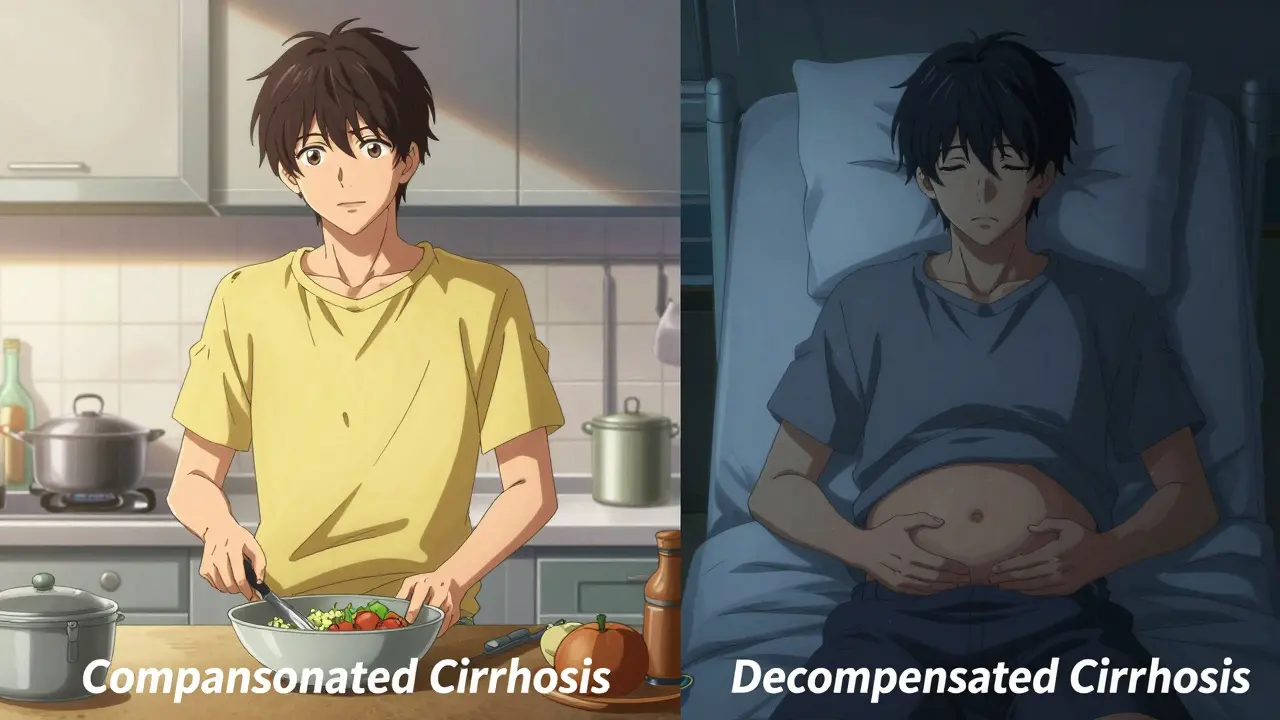
- Compensated Cirrhosis: In this stage, significant scarring exists, but the liver is still able to perform most of its jobs. You might feel fine or experience mild fatigue, but there are no major complications. With proper care, many people live for decades in this stage. Survival rates are high, with 80-90% of patients surviving five years after diagnosis.
- Decompensated Cirrhosis: This is the advanced stage where the liver can no longer cope. Scar tissue blocks blood flow so severely that pressure builds up in the portal vein (portal hypertension), leading to dangerous complications. Symptoms become obvious and severe, including fluid accumulation in the abdomen (ascites), bleeding from swollen veins in the esophagus (varices), and confusion due to toxin buildup in the brain (hepatic encephalopathy). Survival drops significantly here, with only 20-50% of patients surviving five years without a transplant.
The transition from compensated to decompensated is a pivotal moment. It marks the shift from managing a chronic condition to fighting for survival. Early intervention aims specifically to delay or prevent this decompensation.
Common Causes of Liver Scarring
Cirrhosis is not a disease itself but the result of long-term damage from other conditions. Identifying the root cause is crucial because treating the underlying issue can stop the progression of scarring.
| Cause | Description | Prevalence/Trend |
|---|---|---|
| Alcohol Use Disorder | Long-term heavy drinking causes inflammation and cell death. | Historically the leading cause, though declining in some regions. |
| Non-Alcoholic Fatty Liver Disease (NAFLD/NASH) | Fat buildup in the liver leads to inflammation and scarring, often linked to obesity and diabetes. | Rapidly rising; now accounts for ~24% of cases in the US, surpassing alcohol in some demographics. |
| Hepatitis B and C | Viral infections that cause chronic inflammation. | Major global cause; Hepatitis C is now curable with medication, preventing future cirrhosis. |
| Autoimmune Diseases | Conditions like Primary Biliary Cholangitis (PBC) or Autoimmune Hepatitis where the body attacks the liver. | Less common but significant, particularly in women. |
| Genetic Disorders | Such as Hemochromatosis (iron overload) or Wilson’s disease (copper overload). | Rare but treatable if caught early. |
Notice how NAFLD is becoming a dominant driver of cirrhosis. This reflects broader public health trends regarding diet, weight, and metabolic health. If you have type 2 diabetes or obesity, your risk is higher, even if you never drink alcohol.
Diagnosis and Severity Scoring
Because cirrhosis often has no symptoms in early stages, diagnosis frequently happens during routine blood tests or imaging for other issues. Doctors look for elevated liver enzymes, low platelet counts (due to spleen enlargement from portal pressure), and abnormal clotting times.
To determine how severe the disease is and who should get a liver transplant, doctors use specific scoring systems. These tools provide an objective way to compare patients and prioritize care.
- MELD Score (Model for End-Stage Liver Disease): This score ranges from 6 to 40. It uses lab values (bilirubin, INR, creatinine) and sodium levels to predict short-term mortality. A score above 15 indicates significant risk. Higher scores mean you are sicker and move you up the transplant waiting list faster.
- Child-Pugh Classification: This older system categorizes patients into Class A, B, or C based on bilirubin, albumin, INR, ascites, and encephalopathy. Class A is best prognosis (85-100% 2-year survival), while Class C is worst (35-45% 2-year survival).
Imaging plays a huge role too. Ultrasound elastography measures liver stiffness. A value exceeding 12.5 kPa strongly suggests cirrhosis. While liver biopsy was once the gold standard, non-invasive tests are now preferred because they avoid the risks of surgery and provide quick results.
Living with Cirrhosis: Management and Lifestyle
If you are diagnosed with compensated cirrhosis, the goal is to keep it that way. This requires strict lifestyle changes and regular monitoring. There is no pill that reverses existing scar tissue, but you can protect the healthy tissue left.
Dietary changes are immediate and impactful. You must limit sodium to less than 2,000 mg per day to prevent fluid retention. Alcohol must be stopped completely, regardless of whether alcohol caused the cirrhosis, because any additional stress on the liver can trigger decompensation. Protein intake needs careful balancing; too little can weaken muscles, but too much can worsen brain fog in advanced cases. Working with a hepatologist and a nutritionist is key.
Medication management is also critical. Your liver metabolizes drugs differently, so doses often need adjustment. Over-the-counter painkillers like acetaminophen can be dangerous in high doses. Always consult your doctor before taking any new medication, including herbal supplements, which can sometimes be toxic to the liver.
When the Liver Fails: Transplantation
When cirrhosis reaches the decompensated stage and quality of life plummets, or when the MELD score indicates imminent death, a liver transplant becomes the only viable option. According to the United Network for Organ Sharing (UNOS), cirrhosis accounts for about 40% of all liver transplants.
The transplant process is complex. First, you are evaluated for eligibility. Factors like active substance abuse, certain cancers, or severe heart/lung disease might disqualify you. If approved, you join a national waiting list. The wait can take months or years, depending on your blood type, size, and MELD score. Sadly, about 12% of people on the waiting list die before receiving an organ.
Recent innovations are helping. Normothermic machine perfusion allows doctors to assess and repair donor livers outside the body, increasing the number of usable organs by 22%. Additionally, research into bioartificial livers and stem cell therapies offers hope for bridging the gap until a donor organ is available. One study showed hepatocyte transplantation reduced MELD scores by 40% in six months, suggesting potential future alternatives.
Prognosis and Future Outlook
The outlook for cirrhosis depends entirely on the stage at diagnosis and adherence to treatment. For those with compensated cirrhosis who address the underlying cause (e.g., curing Hepatitis C or stopping alcohol), life expectancy can be near-normal. For those who progress to decompensation, the focus shifts to symptom management and transplant evaluation.
The medical field is moving toward precision medicine. Instead of just looking at clinical symptoms, researchers aim to stratify patients by molecular fibrosis signatures within the next five years. New antifibrotic drugs are in trials, targeting the mechanisms of scarring directly. While we cannot yet reverse established cirrhosis, we are getting better at slowing it down and identifying at-risk individuals earlier.
Is cirrhosis reversible?
Established cirrhosis is generally considered irreversible because the scar tissue permanently alters the liver's structure. However, early-stage fibrosis can sometimes be reversed if the underlying cause is treated promptly. Even with cirrhosis, stopping the damage (like quitting alcohol or curing hepatitis) can prevent further scarring and allow the liver to function adequately for many years.
What are the first signs of cirrhosis?
Early cirrhosis often has no symptoms. As it progresses, signs may include extreme fatigue, unexplained weight loss, nausea, and easy bruising. Advanced signs include jaundice (yellowing of skin/eyes), abdominal swelling (ascites), red palms, and confusion or difficulty concentrating (hepatic encephalopathy).
How is cirrhosis diagnosed?
Diagnosis involves blood tests to check liver function and clotting, imaging tests like ultrasound or elastography to measure liver stiffness, and sometimes a liver biopsy. Doctors also calculate MELD or Child-Pugh scores to determine severity.
Can you live a normal life with compensated cirrhosis?
Yes, many people with compensated cirrhosis live normal lives for decades. The key is strict adherence to medical advice, avoiding alcohol, maintaining a healthy weight, and attending regular check-ups to monitor for complications.
What is the success rate of liver transplants for cirrhosis?
Liver transplantation has high success rates. Approximately 70-80% of recipients survive one year post-transplant, and 50-60% survive five years or more. Outcomes depend on the patient's overall health, age, and ability to manage post-surgery medications.
Does fatty liver always lead to cirrhosis?
No. Simple fatty liver (steatosis) does not always progress. However, if it develops into NASH (non-alcoholic steatohepatitis), which involves inflammation, it can lead to fibrosis and eventually cirrhosis over many years. Weight loss and managing diabetes can halt this progression.